Download presentation
Presentation is loading. Please wait.

1
PRESENTER: 江珮甄 SUPERVISOR:
Case presentation PRESENTER: 江珮甄 SUPERVISOR:

2
Identifying information
Name:陳O銘 Gender: male Chart number: 116XX593 Birth date: 2001/10/11 Age: 13y Chief complaint Tea-color urine for two months

3
Present illness 2 months
Intermittent abnormal urine color for more than 2 months (tea color or red) An-Nan Fever up to 39’C , mild nasal obstruction (allergic rhinitis hx) Gross hematuria No other URI symptoms, no dysuria, no frequency, no flank pain, no trauma, no medication, fair appetite and activity U/A: NIT(+) LEU(3+) RBC&WBC > 1000/ul U/C: CONS echo: left renal enlargement, No obvious hydronephrosis, stone, or cyst Impression: Urinary tract infection, hematuria, proteinuria (1261mg/24hrs) 07/30 動畫 7/30 An-Nan susp nephritis transferred for further survey> ER Hematuria with rhinorrhea and nasal obstruction BT:36.9C , HR:70/mm , RR:22/min , BP:112/72 right back mild knocking pain ->Admission PE: Left knocking pain 08/03
 An-Nan. Fever up to 39’C , mild nasal obstruction (allergic rhinitis hx) Gross hematuria. No other URI symptoms, no dysuria, no frequency, no flank pain, no trauma, no medication, fair appetite and activity. U/A: NIT(+) LEU(3+) RBC&WBC > 1000/ul U/C: CONS. echo: left renal enlargement, No obvious hydronephrosis, stone, or cyst. Impression: Urinary tract infection, hematuria, proteinuria (1261mg/24hrs) 07/30. 動畫 7/30. An-Nan susp nephritis transferred for further survey> ER. Hematuria with rhinorrhea and nasal obstruction. BT:36.9C , HR:70/mm , RR:22/min , BP:112/72. right back mild knocking pain. ->Admission. PE: Left knocking pain. 08/03.")
4
Past history Birth History:
G2P2, GA: 40wks, BBW:3400g, DOIC(-), PROM(-) Vaccination: As schedule Growth and Development: BH: cm = 85-97th percentile BW: 46.5 kg = 3rd-15th percentile Developmental milestones: WNL Hospitalized history: several times in chi-mei hospital due to pneumonitis before 10 years old Medication history: anti-histamine Travel history: nil Drug Allergy History: Not known drug allergy history
, PROM(-) Vaccination: As schedule. Growth and Development: BH: cm = 85-97th percentile BW: 46.5 kg = 3rd-15th percentile. Developmental milestones: WNL. Hospitalized history: several times in chi-mei hospital due to pneumonitis before 10 years old. Medication history: anti-histamine. Travel history: nil. Drug Allergy History: Not known drug allergy history.")
5
Family history

6
Physical examination Neck: supple Consciousness: alert
Erythema(-), local heat(-), wound(-), discharge(-), fluctuate(-) Chest: symmetric expansion, subcostal retraction( - ) B.S.: clear,no crackles H.S.: regular heart beat, no murmur Abd: soft, not distended L/S: impalpable / impalpable, No tenderness, No rebounding pain BS: normoactive Left knocking pain(+) No tenderness over suprapubic area Extremities: freely movable, pitting edema (-) Skin: turgor fine, no rash , no ecchymoses or petechiae Consciousness: alert Appearance and activity: fair Vital sign: BT:36.9C, P:65/min, R:20/min, BP:114/81mmHg Head: No scalp lesion conj: not anemic sclera: not icteric throat: not injected Oral: ulcer(-), no bulging mass, no pus discharge eardrum: intact
, local heat(-), wound(-), discharge(-), fluctuate(-) Chest: symmetric expansion, subcostal retraction( - ) B.S.: clear,no crackles. H.S.: regular heart beat, no murmur. Abd: soft, not distended. L/S: impalpable / impalpable, No tenderness, No rebounding pain. BS: normoactive. Left knocking pain(+) No tenderness over suprapubic area. Extremities: freely movable, pitting edema (-) Skin: turgor fine, no rash , no ecchymoses or petechiae. Consciousness: alert. Appearance and activity: fair. Vital sign: BT:36.9C, P:65/min, R:20/min, BP:114/81mmHg. Head: No scalp lesion. conj: not anemic. sclera: not icteric. throat: not injected. Oral: ulcer(-), no bulging mass, no pus discharge. eardrum: intact.")
7
Hematuria ddx 1. UTI 2. Hypercalciuria 3. IgA nephropathy

8
Plan Check CBC/DC, BUN/Cr, Ca/P/Na/K/Cl, AST/ALT, CRP
Check U/A and RBC morphology, U/C, 24 hr urine Ccr & daily protein loss & daily calcium loss Arrange KUB and renal echo Check IgG, A, E, ANCA, anti-GBM, C3,C4 Check HBsAg, anti-HBs Ab, HCV Ab, ASLO Supportive care

9
Lab data(1) 8/7 U/A 8% dysmorphic RBC Dysmorphic RBC
 8/7 U/A 8% dysmorphic RBC Dysmorphic RBC")
10
Lab data(2) 24 hr Urine: TP:29*3050=884 mg Spot urine:
Ca/Cr:0.8/45=0.017<0.2 -> idiopathic hypercalciuria is less likely CCR:89 EGFR:120 24小時尿液, 尿總量3050 mL 08-04 Random urine

11
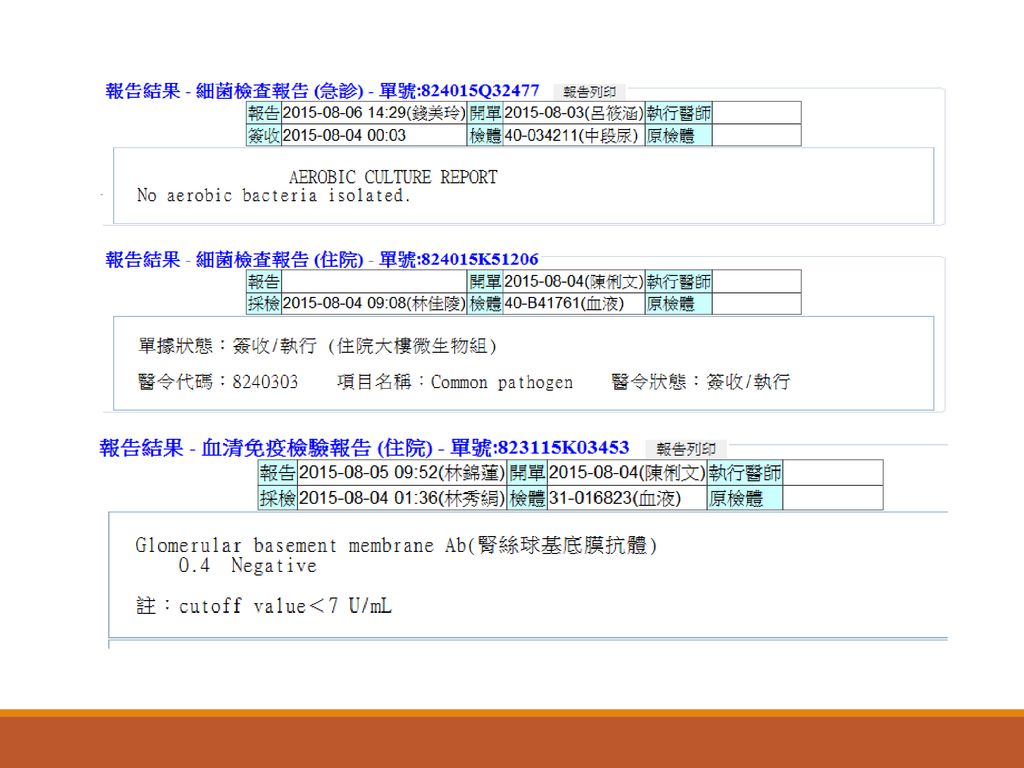
Lab data in AN Nan Lipid profile: TG 111, Chol 167 Serology: mg/dl
HBsAg(-), anti-HBsAb(-), HCV Ab(-), throat swab: (-), U/C: gram postive coccus, 1000CFU/ml Adneovirus:? Cryogolbulin:? ANCA:? B/C? IgG IgA IgE IgM C3 C4 ASLO 908 284 628↑ 116 79.5 17.9 <25 IU/ml
, anti-HBsAb(-), HCV Ab(-), throat swab: (-), U/C: gram postive coccus, 1000CFU/ml. Adneovirus: Cryogolbulin: ANCA: B/C IgG. IgA. IgE. IgM. C3. C4. ASLO ↑ <25 IU/ml.")
13
Renal echo

14
Image Kub Film of chest PA view shows: Film of KUB shows:
1. Normal configuration of the spine. 2. Nonspecific bowel gas pattern. 3. No abnormal calcification is noted. 蔡依珊醫師-放診專 682 1. The size of heart and mediastinum show normal. 2. No active pneumonia patch. 3. Both CP angles are sharp.

15
Tentative diagnosis 1. glomerulonephritis

16
Management Enalapril 5mg/tab (Sintec) 1 tab QD PC for proteinuria
Dipyridamole75mg/tab (Dipyridamole)1 tab BID ->prevention of glomerular thrombosis OPD follow up
1 tab BID ->prevention of glomerular thrombosis. OPD follow up.")
17
Disscussion Evaluation of gross hematuria in children

18
Uptodate: Evaluation of gross hematuria in children

19
ETIOLOGY most commonly identified etiologies for gross hematuria in children urinary tract infection (UTI) perineal or urethral irritation trauma acute nephritis coagulopathy stone no etiology

21
ETIOLOGY Glomerular Nonglomerular IgA nephropathy Alport syndrome
hypercalciuria cystitis Sickle cell trait

23
glomerulonephritides
Primary GN - IgA nephropathy bacterial tonsillitis, or by other viral upper respiratory infections - Membranoproliferative glomerulonephritis (MPGN) hepatitis C and B viral infections - Anti-glomerular basement membrane (GBM) disease Anti-GBM antibody - Idiopathic crescentic GN
 hepatitis C and B viral infections. - Anti-glomerular basement membrane (GBM) disease. Anti-GBM antibody. - Idiopathic crescentic GN.")
24
glomerulonephritides
Secondary GN - Poststreptococcal GN (PSGN) anti-streptolysin ASO(+) A history of pharyngitis or impetigo (two or three weeks prior to onset of hematuria) - Henoch-Schönlein purpura (HSP) Palpable purpura of lower extremities, abdominal pain, hematochezia, arthralgias - Systemic lupus erythematosus nephritis(SLE) Butterfly rash, polyserositis, hematologic abnormalities - Alport ‘s disease family history of hematuria, kidney disease ,hearing loss 在兒童常見的是 Anaphylactoid purpura(Henoch-Schönlein purpura)。大多 會嚴重腹痛與關節痛,並且在下肢的伸展側、屁股出現出血性的紫斑、血 管炎,大概 50%會造成腎臟的疾病 。Anaphylactoid purpura 有一半的機率 會造成腎臟傷害,少部分還會造成腎衰竭。
 anti-streptolysin ASO(+) A history of pharyngitis or impetigo (two or three weeks prior to onset of hematuria) - Henoch-Schönlein purpura (HSP) Palpable purpura of lower extremities, abdominal pain, hematochezia, arthralgias. - Systemic lupus erythematosus nephritis(SLE) Butterfly rash, polyserositis, hematologic abnormalities. - Alport ‘s disease. family history of hematuria, kidney disease ,hearing loss. 在兒童常見的是 Anaphylactoid purpura(Henoch-Schönlein purpura)。大多. 會嚴重腹痛與關節痛,並且在下肢的伸展側、屁股出現出血性的紫斑、血. 管炎,大概 50%會造成腎臟的疾病 。Anaphylactoid purpura 有一半的機率. 會造成腎臟傷害,少部分還會造成腎衰竭。")
25
Indication of Renal Biopsy
Unexplained acute renal failure or chronic renal insufficiency Acute nephritic syndromes Unexplained proteinuria and hematuria Previously identified and treated lesions to plan future therapy Systemic diseases associated with kidney dysfunction, such as SLE, Goodpasture's syndrome, and Wegener's granulomatosis, to confirm the extent of renal involvement and to guide management Suspected transplant rejection, to differentiate it from other causes of acute renal failure

26
Thank you for your attention!!

27
Asymptomatic hematuria
No identifiable cause – 36 percent ● Hypercalciuria – 22 percent ● IgA nephropathy – 16 percent ● Poststreptococcal glomerulonephritis – 7 percent ● Other glomerulopathies including thin basement membrane disease – 2 percent ● Congenital anomalies (eg, ureteropelvic junction obstruction or renal dysplasia) – 2 percent ● Sickle cell trait – 1 percent
 – 2 percent. ● Sickle cell trait – 1 percent.")
30
The Massachusetts General Hospital Handbook of Internal Medicine 5/e

31
hematuria >5 RBCs / HPF –unspun urine
1~2 RBCs / HPF – centrifuged urine Traumatic vs Non-traumatic Non-traumatic -Upper GU RBC casts, dysmorphic RBCs, proteinuria with microscopic hematuria -glomular -nonglomular -lower GU

32
Nontraumatic bleeding
Lower GU tract: Suprapubic pain and dysuria Urgency, frequency, pyuria and bacteriuria URI S/s, fever, suprapubic tenderness – viral cystitis – resolved within 5~7 days Urethral foreign body Urolithiasis Drugs: cyclophosphamide

33
Upper GU tract: Glomerular
Edema, hypertension, oligouria Hx of pharyngitis or impetigo in previous 2 weeks poststreptococcal glomerulonephritis URI in 1~2 days IgA nephropathy, hereditary nephritis Family hx of deafness + renal disease Alport’s syndrome Palpable purpura of lower extremities, abdominal pain, hematochezia, arthralgias HSP Butterfly rash, polyserositis, hematologic abnormalities SLE

34
Upper GU tract:Nonglomerular
Sickle cell trait Wilms’ tuor (10%) Polycystic kidney, renal hemangioma, hydronephrosis Idiopathic hypercalciuria- family history
 Polycystic kidney, renal hemangioma, hydronephrosis. Idiopathic hypercalciuria- family history.")
35
Diagnoses: Must confirmed by microscopy Contamination by menstruation
Pigmenturia RBC morphology: For nonglomerular hematuria For glomerular hematuria: Idiopathic hypercalciuria: Spot urine Ca/Cr>0.21 24hr-Urine Ca: > 4mg/kg/day

36
Proteinuria

37
Proteinuria the amount of protein (nephrotic or non-nephrotic) the type of protein (albuminuria or low molecular weight proteinuria) underlying pathological damage (glomerular vs non-glomerular) Most cases of proteinuria can be classified as tubular, overflow, or glomerular 1.什麼型態:如因腎絲球的通透性改變則流失的尿白質大都屬一些分子量較大的蛋白質;如免疫球蛋白(IgG),白蛋白等。如發現尿液中的蛋白質為胺基酸或一些腎小管分泌的蛋白質,則可知腎小管出現了異常。有些惡性腫瘤如多發性骨髓瘤等,則因製造太多免疫球蛋白而從腎臟流失。以上各種不同型態的蛋白質可藉電泳分析,定性定量分析等而有所診斷。 2.多少量:每天的尿蛋白流失量如少於1公克屬輕度,3公克以上屬重度(如腎病症候群),介於1到3公克之間則屬中度。腎臟如每天的尿蛋白總量愈多則受害情形愈嚴重且預後愈差,但仍有例外的情形。在此特別強調的是:單一次的尿液檢查並無法準確的判斷腎臟的受害程度。 3.什麼情況出現:發燒或劇烈運動後,因腎臟血流量會增加而出現「暫時性」的蛋白尿。另外有一種蛋白尿僅發生於白天走動時而晚間睡眠時段則正常,我門稱之為「端坐型」;好發於小於卅歲的年輕人。不管走動或躺下,蛋白質的流失量皆異常時,我們稱之為「持續型」;這一類的蛋白尿在臨床較有意義。
 Most cases of proteinuria can be classified as tubular, overflow, or glomerular. 1.什麼型態:如因腎絲球的通透性改變則流失的尿白質大都屬一些分子量較大的蛋白質;如免疫球蛋白(IgG),白蛋白等。如發現尿液中的蛋白質為胺基酸或一些腎小管分泌的蛋白質,則可知腎小管出現了異常。有些惡性腫瘤如多發性骨髓瘤等,則因製造太多免疫球蛋白而從腎臟流失。以上各種不同型態的蛋白質可藉電泳分析,定性定量分析等而有所診斷。 2.多少量:每天的尿蛋白流失量如少於1公克屬輕度,3公克以上屬重度(如腎病症候群),介於1到3公克之間則屬中度。腎臟如每天的尿蛋白總量愈多則受害情形愈嚴重且預後愈差,但仍有例外的情形。在此特別強調的是:單一次的尿液檢查並無法準確的判斷腎臟的受害程度。 3.什麼情況出現:發燒或劇烈運動後,因腎臟血流量會增加而出現「暫時性」的蛋白尿。另外有一種蛋白尿僅發生於白天走動時而晚間睡眠時段則正常,我門稱之為「端坐型」;好發於小於卅歲的年輕人。不管走動或躺下,蛋白質的流失量皆異常時,我們稱之為「持續型」;這一類的蛋白尿在臨床較有意義。")
38
Proteinuria Albumin: creatinine ratio Protein: creatinine ratio
ACR/PCR elevation: glomerular or tubular disease DM Heavy metal Amyloidosis Multiple myeloma Congestive heart failure

39
Approach Considerations
orthostatic proteinuria Urine microscopy Split urine collection - Daytime (7 am to 11 pm) and overnight (11 pm to 7 am) Glomerular proteinuria Urine microscopy – To search for dysmorphic red blood cells and casts Urine collection (24 h) for quantification of albumin (or protein) excretion and creatinine clearance Serum creatinine, albumin, cholesterol and blood glucose Autoantibody determinations - If indicated, including antistreptolysin O titers, antinuclear antibodies (ANAs), anti-DNA antibodies, complement levels, and cryoglobulins Hepatitis B, hepatitis C, and HIV serologies - If indicated Urine and plasma protein electrophoresis - If indicated Anti–glomerular basement membrane (anti-GBM) antibodies and antineutrophil cytoplasmic antibodies (ANCA) – If there is a suspicion of pulmonary renal syndrome.
 and overnight (11 pm to 7 am) Glomerular proteinuria. Urine microscopy – To search for dysmorphic red blood cells and casts. Urine collection (24 h) for quantification of albumin (or protein) excretion and creatinine clearance. Serum creatinine, albumin, cholesterol and blood glucose. Autoantibody determinations - If indicated, including antistreptolysin O titers, antinuclear antibodies (ANAs), anti-DNA antibodies, complement levels, and cryoglobulins. Hepatitis B, hepatitis C, and HIV serologies - If indicated. Urine and plasma protein electrophoresis - If indicated. Anti–glomerular basement membrane (anti-GBM) antibodies and antineutrophil cytoplasmic antibodies (ANCA) – If there is a suspicion of pulmonary renal syndrome.")
41
Non-glomerular Glomerular

44
Clinical information:
1.Right renal size:12.37cm X4.83cm Left renal size:12.94cm X4.72cm Both renal size are larger than normal limit 2.Bilateral cortical thickness are within normal limit. 3.Bilateral parenchymal density are higher than normal limit. 4.Bilateral renal pelvicalyceal system are not dilated. No hydroureter is noted. 5.No stone or occupied mass lesion can be found. 6.The bladder is well distended with smooth mucosa, except full with floating material. 7.No obvioius renal vascular disorder: right RI:0.73; left RI:0.62 Diagnosis: Renal parenchymal disorder, cause unidentified Examer: Yuan-Yow Chiou/ Yuan-Yow Chiou

Similar presentations













 ;而另一些 事件則會受到該事件現階段的狀況影響。>")


 來判斷是否為場景變換,以方便使用者來 找出所要的片段。>")
 參考資料:疾病管制局 http://www.cdc.gov.tw.>")

 一種質性資料, 其觀察值可歸類於數個不相交的項目內, 例 : 性別, 滿意度, …, 一般以各項的統計次數表現. 分析此種資料,通常用卡方檢定 類別資料分析 ----- 卡方檢定 卡方檢定基本理論 一個含有 k 項的試驗,設 p i.>")
 醣類 礦物質與維生素(少量)>")

來描述一般物價持續上升的現象,而物價膨脹率(inflation rate)為物價水準的變動百分比。>")
>")
 ,用樣本 s 來取代 因為用 s 來估計 ,所呈現出來的分佈已不 是 z distribution ,而是 t distribution.>")
 蛋白質純化 學生 : 陳建良 2004.11.02.>")
